How Can We Help?
Case Study
Overview
Presenting problem/request of each party
‘You are our last hope as a family, we have been to many other people but nothing helps’. When a session starts with these words it is easy to feel helpless and hopeless before you begin. The full weight of responsibility has moved immediately from the family to the practitioner and a sense of impotence appears. This was prophetic and achieving an effective balance of authority and responsibility would be a central characteristic of this case.
The family comprised mother, Lynne, father, Raymond and two children, 11-year-old Millie and her sister, Anne who was 9. At the beginning of the first session each was asked for their request of therapy. Millie, as the person who had been identified as having the presenting problem wanted the family to be happier, her sister did not want to be ’pressured as much’, Lynne requested less screaming in the house while Raymond wanted to build more resilience to cope with the family crises.
The family had been referred by their GP who had also worked with the family but now believed the issues required more specialist intervention. He had identified Millie as the ‘patient’ and asked for help for the family to address her anxiety and depression. The parents explained that their children screamed at them and refused to comply with ordinary parenting requests with getting ready for school and evenings being particularly difficult. Raymond said that he found parenting ‘very stressful’ while Lynne expressed guilt about the children’s behavioural problems saying her psychiatrist had blamed her for the difficulties and she was struggling to redress her failings. When disciplined Millie would threaten to harm herself and in the past, she had made attempts to jump out of a moving car and scratched at her skin with paperclips. Anne had been diagnosed with ADHD and the family had sought referral for an assessment for Millie for this condition.
Social system presenting to session
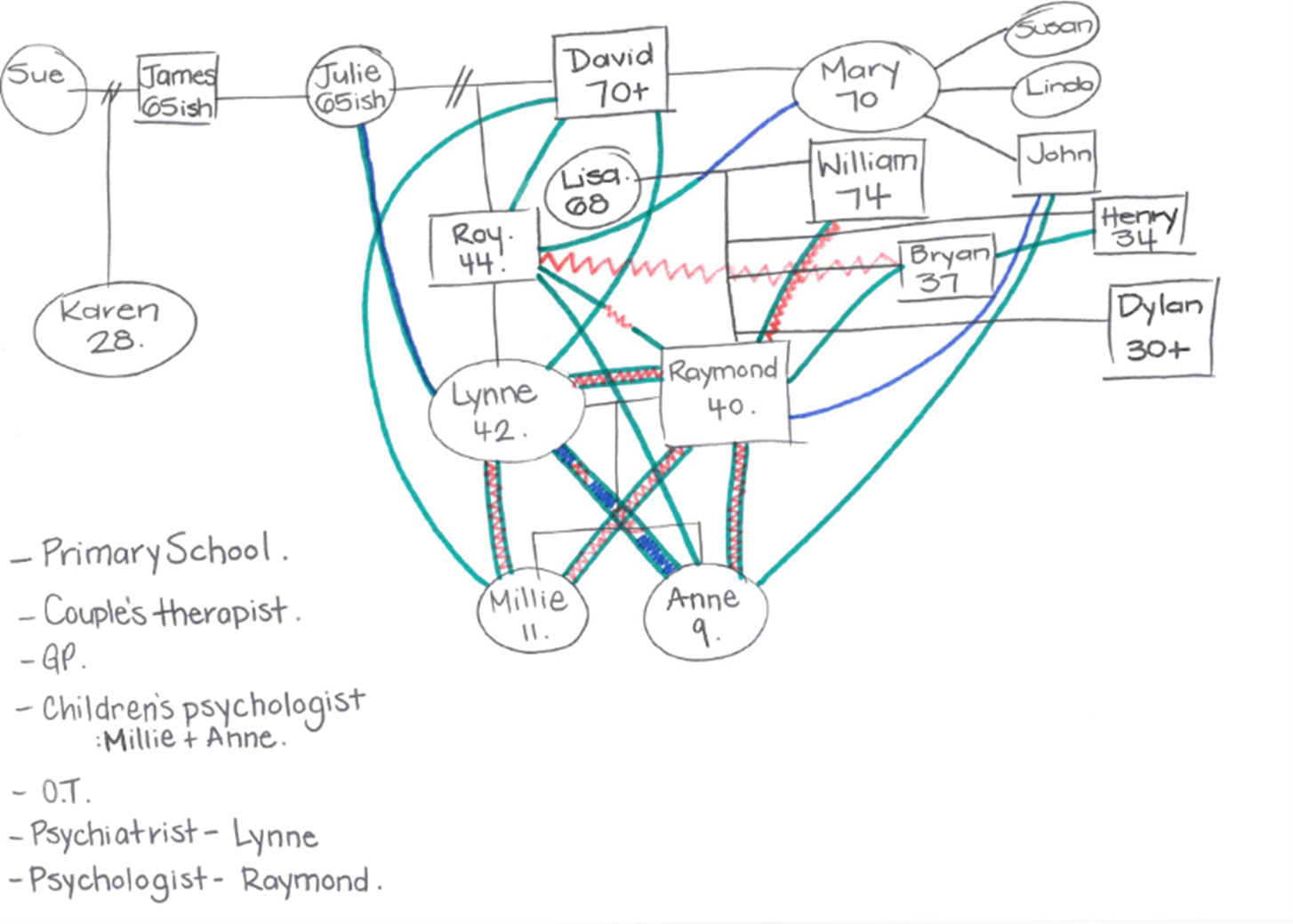
The family presented together at the first visit, but others comprised their social network who were not physically present but influential. This included both parent’s family of origin, their workplace, school, the GP, both children’s psychologist, an occupational therapist Lynne’s psychiatrist, Raymond’s psychologist, and a couple therapist.
Ecogram
Analysis using Bower Place Model
Politics
The family described a pattern of interaction which reflected a split between authority and responsibility, between the parents and between the family and helper system. In the session Millie explained that her father spent all his time on his computer which resulted in a distressing argument between father and daughter that looked more like a sibling conflict than that between parent and child. Raymond became verbally abusive and defensive, and Millie distressed as she attempted to defend herself while Lynne looked helpless, and Anne moved close to her sister and attempted to comfort her. In unpacking this interaction, they spoke of a repetitive pattern where Raymond would either abnegate all responsibility for parenting saying he ‘was no good at it’ and withdraw to his computer or engage in verbally abusive exchanges with the children which Lynne felt compelled to diffuse.
This pattern was replicated in the wider system where Lynne would leave the family and seek support from her parents when the conflict escalated. The whole family looked to professionals to ‘solve the problem’ and appeared impotent to effect change within the relationships.
Time
The family reported that they had ‘always’ experienced difficulties and differences in their parenting styles and that both children had been difficult and unsettled infants. Anne had been very active and distractible and had attracted an ADHD diagnosis at 7years old.
The couple had separated for six months in the year before they attended therapy but decided to continue their relationship as they ‘wanted to be a family’.
Lynne’s brother, Roy who was two years older than her had an intellectual disability because of a car accident he sustained when Millie was 2 years old. He was very close to his sister who he would turn to when distressed. In recent years this had become more frequent and when Roy called, Lynne felt compelled to go to him to help him resolve the issue, leaving Raymond to manage the children.
Lynne was highly regarded in her occupation as a family lawyer and had been acknowledged and promoted in the past year. By contrast Raymond, who worked in an administrative role said he was not ambitious and had remained at the same level for the past 10 years.
Space
Inside Space
Raymond spoke of feeling overwhelmed and incompetent in his role as parent. He had also been diagnosed as ‘being on the autism spectrum’ which he interpreted as meaning he was unable to effectively parent his children and form a close relationship with his eldest daughter. An incident was reported where he had become overwhelmed by the demands of his children and had spent half an hour banging his head which had required Millie to manage him.
Lynne descried feeling unsupported and guilty about the family’s state and saddened by her inability to change the situation. She said she felt ’upset’ much of the time.
Millie expressed distress at her father’s conduct towards her and said, ‘anger and sadness get mixed up’ and then she would threaten to harm herself. She spoke of being worried about her mother and fearing her father ‘loves his computer more than me’.
Anne would withdraw in the face of the family conflicts but was also ‘worried and sad’ for Millie who she would attempt to comfort when conflict erupted. It was reported that she would often be awake and wandering the house at 2.30am and was regularly awake by 4.00am.
Outside Space
It was reported that Millie would fracture with everyone in the family leaving her isolated but most often, and dramatically conflicting with her father. At these times she would threaten to harm herself which drew her mother close and further alienated Raymond who viewed this behaviour as manipulative. As these episodes often occurred at night Lynne would sit with Millie for hours to help her calm down or alternately leave the family to seek support from her parents when she became too distressed. They took the view that Raymond was a poor parent and partner and urged Millie to leave him.
A second pattern was also identified which was less frequently but was more positive. This was one where Millie’s misbehaviour was met by a calm and coherent response by her parents which resulted in greater closeness with her father and a de-escalation in her distress and oppositional behaviour.
The family appeared relatively isolated with more time spent with professionals than friends.
Development
The parents were both in their early 40’s and managing competing demands of career and family responsibilities. The girls were in middle childhood at a stage where they would be expected to be moving beyond the boundary of the family and forming meaningful friendships with same sex peers and focussed on school and external hobbies and interests.
As a family they were at a stage where the primary focus was still within the family with children beginning to make independent relationships that would also draw others into the family.
Neither child or Raymond reported having friends and while Lynne had work colleagues with whom she had ‘friendly interactions’ she too did not have close friends.
Constraints
A primary constraint was the competing definitions of the children’s and adult’s behavioural issues. Having consulted professionals for much of the children’s lives they had collected individual diagnoses which located difficulties inside as opposed to outside each person and as part of their interactional pattern. They constantly sought ‘outside’ help, either in the form of medication, professional advice or from Millie’s parents.
The belief that the difficulties were constitutional rather than environmental fuelled their sense of impotence, guilt and helplessness and created conflict in the therapeutic relationship when Millie was diagnosed with depression and medication advised.
Another constraint was the isolation in the family and lack of relationship with other families at a similar life stage who could provide support and ordinary conversation and parenting advice.
Finally, the fracture between Raymond and his in-laws and their willingness to provide support to Lynne in the context of their conflict was another constraint.
Advice
At the conclusion of the first visit the care and affection and desire to be close to each other was acknowledged but also the anger and sadness and blame they each carried for the problems. We noted that when there was shouting and yelling people became worried and this worry made people hurt, angry, and sad and then they behaved badly. This was described as the ‘anti-pattern’. The antidote to this was the alternate pattern, a pattern of kindness and control which was self-generating. The anti-pattern had been mapped in the session and the family were tasked with drawing the alternate, safe pattern and to notice how adding kindness changed relationships.
Follow Up
The theme of the two patterns shaped the work done with this family and a year later positive changes had appeared. Raymond and Lynne formed a stronger parenting subsystem and were able to respond to their daughter’s refusal to co-operate and subsequent distress in a clear, firm and less emotional way. Lynne stopped turning to her parents for support when in conflict with her husband and the couple were better able to resolve differences between them. She also stopped stepping between her husband and daughter when they conflicted. As these changes unfolded the relationship between father and daughter improved with Lynne reporting that Raymond was more supportive and understanding of Millie while he noted he was less critical and was spending time together playing computer games. Millie’s threats of self-harm stopped. Lynne attributed the positive changes to the help they were giving other, listening to each other and the children being aware their parents were ‘on the same side’. She also noted that Raymond had been more willing to help and do more practical tasks without being asked.
Explanation given to client
The primary explanation was one that challenged the family’s ‘inside’ view that the difficulties were primarily a function of individual ’sickness’ which carried with it a sense of inevitability and hopelessness to one that focussed on the pattern of interaction between them. It also emphasised the need for the adults to first take responsibility for change with the expectation that the children would follow.
Unique theoretical analysis of key presenting issue
Cessation was the key underpinning idea in analysis of this case. This was cessation at both the level of the macro pattern, the vicious cycle, but also the components of that pattern. The family members were asked to stop unkindness which translated into a series of changes to behaviours, affect and beliefs about themselves and each other.
A second key idea was the proper balance of authority and responsibility with responsibility for change being firmly and appropriately located in each family member dependent on their developmental stage. This meant the practitioner took responsibility to manage the therapeutic process but did not promise to ‘make anyone change’.