How Can We Help?
Children and the Cycle of Dysregulation
In recent years Bower Place has seen an increase in referrals for children whose behaviour is seriously dysregulated resulting in difficulties within the family and the wider community. Dysregulation may be internalized and present as anxiety and depression or externalized as acting out and behavioural problems. These children attract a range of diagnoses including oppositional defiant disorder, post traumatic stress disorder, autism spectrum disorder and major anxiety and depression. These labels encourage practitioners to become focussed on the child as the source of both the difficulty and its resolution. However the literature is clear that the incapacity of the child to manage their strong emotions is often embedded in a family or wider world that also struggles to manage powerful feelings. Attention to the family makes sense, but how best to harness the resources of the group to help a child?
Working with these children in the Bower Place Complex Needs Clinic, has provided the opportunity to develop both skill and expand knowledge in this domain. Our challenge has been to familiarise ourselves with the literature and using this as a foundation to integrate our systemic approach of the Bower Place Method. It is generally agreed that the capacity to control the expression of emotion, neither exploding nor imploding, develops in early childhood and has life –long implications. Authors have researched both intrinsic and extrinsic factors and recognise that each interact with the other. There is little doubt that children are born with their own level of reactivity to their environment a feature of temperament, which is present at birth and is a relatively stable. The child’s capacity to regulate emotional reactivity is a result of increased cognitive control including attention, inhibitory control and executive function. However no child grows up in a vacuum and from birth are in relationship with carers. Studies have demonstrated that securely attached children internalize effective emotion regulation strategies within the relationship which can then be applied outside in other contexts. It has also been shown that maltreated children demonstrate poor emotion regulation and understanding.
As systems and contextual thinker we were eager to identify a different way of conceptualizing and responding to this and map the pattern of interaction that unfolds between all those involved. Like all recursive interactions, it is an endless cycle with no beginning or end, in which each person’s actions fuel that of others and where each feels driven by the other and impotent to effect change on their own behalf.
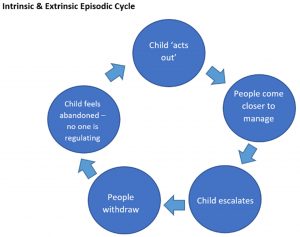
As words are linear we need to start the description at one point in the cycle and the obvious place is the point at which the child demonstrates the ’problem’ behaviour. This may be an externalizing response with tantrums, screaming swearing and threatening or an internalized response like anxiety, fear or despair. The behaviour elicits a response in the parent or carer who comes close in an attempt to resolve the difficulty. When this fails to produce the desired result and in fact escalates the behaviour, the adult withdraws in anger or despair and themselves feels helpless and dysregulated. At this point the child is effectively abandoned with their out of control feelings. Eventually the situation calms but effectively no-one is close enough to regulate the child’s emotions or support them to self-regulate. Inevitably an event will occur where once again the child is unable to manage themselves and the pattern repeats. Every time it does so it entrenches each person’s experience of impotence and inability to exercise effective and appropriate control of themselves, the child or their world.
Understanding and mapping pattern provides a starting point for the practitioner to intervene. It places the difficulty outside the child and allows each person to begin to explore the possibilities available to them to change the pattern and their willingness to take responsibility to do so.
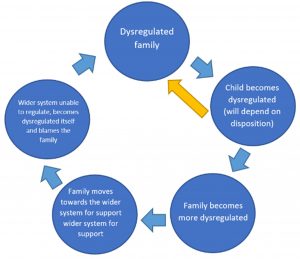
While this pattern describes the individual incidents which produce episodes of dysregulation we were also eager to identify the process by which this pattern develops in a family and the way family members and those engaged to help become caught in its thrall. Bringing together both the inside and outside we hypothesise a circular process where by a child with a reactive temperament is born into a regulated or dysregulated family. The more dysregulated the family the less the child learns to regulate and the more out of control is the family. This cycle spirals more rapidly the less regulated are the parents. However a highly reactive infant may well spiral the family into dysregulation. In time the cycle grows until the family seeks support from helpers or their child’s behaviour draws in wider system. The process that initially occurred between child and family is then replicated between the family and helpers with the system itself becoming dysregulated around the situation which then further escalates the family’s experience of being out of control. Just as the child may internalise and become withdrawn, anxious and inexpressive or angry and inappropriately expressive, so do parents and those engaged to help.
The dysregulation therapists are most likely to suffer is compassion fatigue, a state of chronic physical and emotional exhaustion. Common signs include trouble sleeping, amplified or exaggerated physical reflex, increased emotional reactivity (i.e., irritability, anxiety), hypervigilance and diminished interest in regular activities. It stems from secondary exposure to trauma or suffering presented by clients. The practitioner may become negative towards work, life and others outside the therapeutic relationship, including their own family. They may depersonalize their them as less than human, resulting in reduced quality of service and loss of respect.
How Do we work with these Children and their World?
Having identified the difficulty how do we tailor services to meet the specific needs of this client group? Our first step was to align our own thinking, so we conceptualized the presentation of the children from a broad systemic perspective and not a skin-bound problem to be addressed with the individual who ‘shows’ the problem. In reviewing the literature it is clear that these children and their families require help to Identify, recognize and name emotion, connect feelings with bodily sensations, regulate and express emotions in a socially acceptable way. In order to do this it is crucial that the politics of the case are addressed because unless struggles over ownership, who rightly exercises authority and who will take responsibility to do so, are resolved no change will be long lasting. This struggle must be resolved between the family and the wider system, between the adults with authority in the family and between parents and children. This requires the proper apportioning of authority and responsibility, dependent on each person’s official role and developmental age and stage.
Our next challenge was to identify the best way to do this. What was clear was that ‘traditional’ therapy rooms that are essentially designed for adults, do not suit the needs of these children and their families and in fact may feed the dysregulation. In recognition of this, Bower Place has now created a purpose built room for these children and families. Its design has been guided by the theoretical understanding of the needs of our client group in terms of the management of light, space, sound and colour and also by feedback from those who will access the space. The room aims to be a safe, bounded space with room to move, which provides a range of activities appealing to children and young people. This includes a chalk board painted on the wall, a dolls house, table and chairs for drawing and activities, a basketball hoop, soft toys and games. While it looks like a traditional play room the intent of the room is very different. This is a context where the practitioner can guide the child to show and speak about difficult and painful matters and to demonstrate to the trusted adult the events that are or have occurred in their life and how this manifests in their actions and those of others around them. It give an opportunity for the practitioner to help the child and key family members to Identify, recognize and name emotion, connect feelings with bodily sensations, regulate and express emotions in a socially acceptable way.
Given the centrality of managing issues of ownership and our conceptualization that the difficulty is not located in the child, it is also a place where families can meet in a relaxed fashion to address the family relationship issues which are impacting on their children. The second half of the room provides seating for whole families to engage in family therapy sessions. Furniture is comfortable and easy to move and allows for children to sit close to parents or move freely in and out of session. Our experience is that meeting the needs of all ages enhances the willingness and capacity of family members to explore the factors which are fuelling their struggles and the opportunity to develop individual and interpersonal capacity to address them with the support of those who love them. It is also a time to properly align authority and responsibility.
Managing the space requires confidence and clarity by practitioners. It is important that rules governing the use of the toys and equipment are clearly articulated and supported by parents and caregivers. Children should not be allowed or encouraged to behave in ways that will produce censure at home or in the outside world and setting and reinforcing rules is a valuable opportunity for the practitioner to model calm and appropriate limit setting that does not produce the dysregulated cycle with which the family is so familiar. It can be both shocking and enlightening for parents to watch their child effectively manage their anger, disappointment or fear with the help of a calm adult.
The room is clearly designated as an emotional work space and therefore should not be used a room for child care. It is a place where both adults and children confront the most difficult issues in their lives with the guidance, help and support of another adult who is not frightened by strong emotions.